
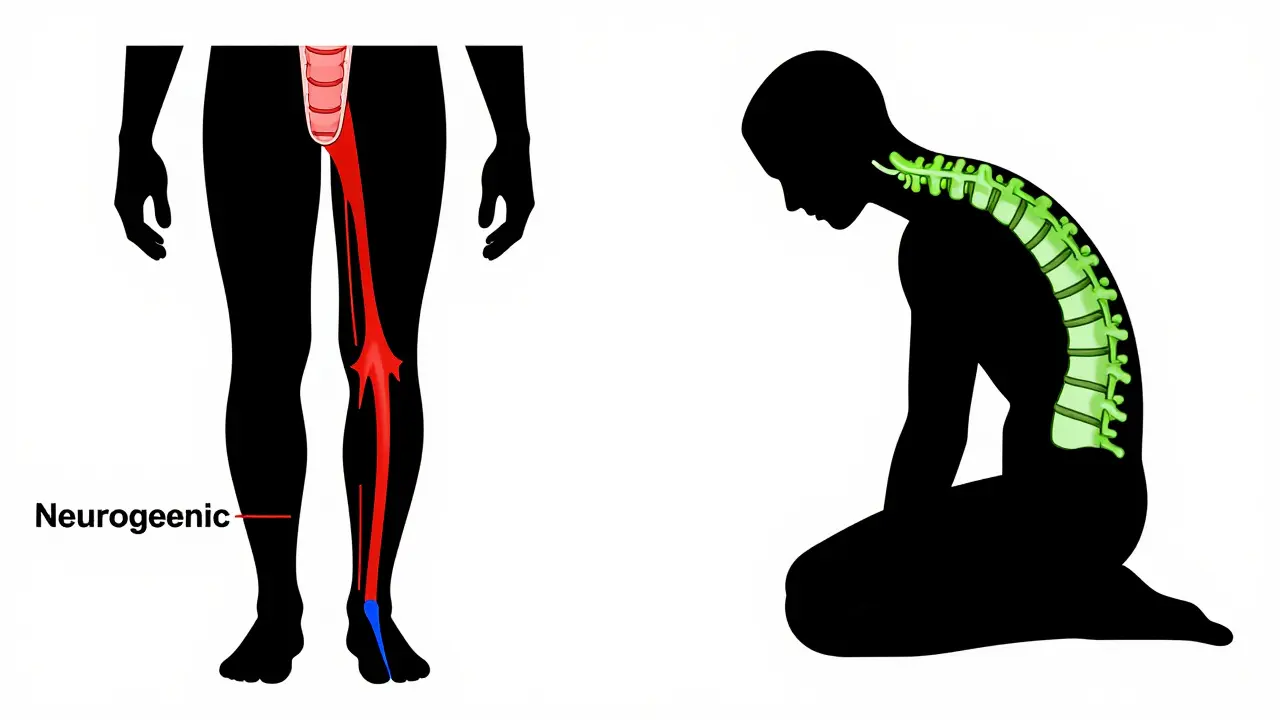
Imagine walking down the street and suddenly your legs feel like lead. You aren't out of breath, but your thighs burn, tingle, or go numb. The only thing that helps? Leaning over a shopping cart or sitting down immediately. If this sounds familiar, you might be experiencing neurogenic claudication, which is a condition caused by compression of the nerves in the lower spine, leading to pain and weakness in the legs during activity. It’s not just "bad knees" or being out of shape. It’s a specific signal from your nervous system that needs attention.
What Is Neurogenic Claudication?
At its core, neurogenic claudication is the hallmark symptom of lumbar spinal stenosis, which is a narrowing of the spinal canal in the lower back that puts pressure on the spinal cord or nerve roots. Think of your spinal canal as a tunnel. Over time, due to aging, arthritis, or injury, that tunnel gets smaller. When you stand up straight or walk, the space shrinks further, pinching the nerves that run down your legs. This pinch causes ischemia (reduced blood flow) and mechanical irritation, resulting in pain, heaviness, or weakness.
The key here is the trigger. Unlike general back pain, which might hurt all the time, neurogenic claudication is positional. It happens when you extend your spine (stand upright or lean back). It goes away when you flex your spine (sit or bend forward). This distinction is crucial because it separates nerve-related pain from other issues like vascular problems or muscle strains.
The Shopping Cart Sign: A Telltale Clue
Have you ever noticed yourself leaning heavily on a walker or a grocery cart while shopping? In the medical world, this is called the shopping cart sign, which is a clinical indicator where patients experience relief from leg pain by leaning forward, often supported by a cart or walker. It’s one of the most reliable signs of neurogenic claudication.
When you bend forward at the waist-usually between 20 and 40 degrees-you open up the spinal canal slightly. This relieves the pressure on the nerves. Patients often describe feeling like they have to "pause and sit" every few blocks. Some even adopt a stooped posture, known as the "simian stance," just to keep moving without pain. If you find yourself naturally hunching over when you walk long distances, take note. It’s your body’s way of seeking relief.
Neurogenic vs. Vascular Claudication: Know the Difference
This is where things get tricky, and misdiagnosis is common. There are two main types of claudication:
- Neurogenic Claudication: Caused by nerve compression in the spine. Pain is relieved by bending forward or sitting. Foot pulses (blood flow) are normal.
- Vascular Claudication: Caused by poor blood circulation in the legs (peripheral artery disease). Pain is relieved by stopping and resting, regardless of position. Foot pulses are weak or absent.
Why does this matter? Because the treatments are completely different. If you treat a nerve problem with heart medication, nothing will happen. If you treat a circulation problem with back surgery, you’re missing the real issue. Doctors look for strong, symmetric foot pulses to rule out vascular causes. If your pulses are fine but your legs still ache when you walk, it’s likely neurogenic.
| Feature | Neurogenic Claudication | Vascular Claudication |
|---|---|---|
| Cause | Nerve compression (Spinal Stenosis) | Poor blood flow (Peripheral Artery Disease) |
| Relief Position | Bending forward, sitting, lying down | Stopping activity (any position) |
| Foot Pulses | Normal and strong | Weak or absent |
| Sensation | Numbness, tingling, burning | Cramping, fatigue, coldness |
| Walking Distance | Variable; improves with flexion | Consistent distance before pain starts |
Diagnosing the Problem
There is no single blood test for neurogenic claudication. Diagnosis relies on your history and physical exam. Your doctor will ask specific questions: "Does bending forward help?" "Do you use a shopping cart to walk longer?" "Is the pain in both legs or just one?"
Imaging plays a confirmatory role. An MRI is the gold standard for viewing soft tissues like discs and nerves. However, here’s a catch: many people over 50 have narrowed spines on an MRI but no pain at all. So, doctors don’t just look at the scan; they match the scan findings with your symptoms. If the MRI shows severe stenosis but you have no leg pain, you might not need treatment. If the MRI shows mild stenosis but you have severe symptoms, further investigation is needed.
Physical exams may include checking your reflexes, strength, and sensation. A simple test like the "five repetitive sit-to-stand" can also assess functional impairment. If you take more than 10 seconds to do five sit-to-stands, it may indicate significant mobility issues related to your condition.

Treatment Pathways: From Conservative to Surgical
Treating neurogenic claudication usually follows a stepwise approach. Most people start with conservative care, and many find lasting relief without ever needing surgery.
1. Physical Therapy and Exercise
This is the first line of defense. The goal isn’t to "fix" the bone structure but to improve how you move. Flexion-based exercises are key. These include:
- Knee-to-chest stretches: Lying on your back and pulling your knees toward your chest opens the spinal canal.
- Hamstring stretches: Tight hamstrings pull on the pelvis, worsening back extension.
- Aerobic conditioning: Stationary biking is excellent because it keeps you in a flexed position while building endurance.
Consistency matters. Studies show that structured exercise programs can significantly improve walking distance and quality of life. Don’t expect overnight results; give it 6 to 8 weeks of regular practice.
2. Medications and Injections
Pain relievers like NSAIDs (ibuprofen, naproxen) can reduce inflammation around the nerves. For more targeted relief, doctors may recommend epidural steroid injections. These involve placing anti-inflammatory medicine directly into the spinal canal near the affected nerves. While not a cure, they can provide months of relief, allowing you to participate more effectively in physical therapy.
3. Surgery: When Conservative Care Fails
If you’ve tried physical therapy, medications, and injections for several months with little improvement, surgery might be the next step. The most common procedure is a laminectomy, which is a surgical procedure to remove part of the vertebral bone (lamina) to create more space for the nerves. This decompresses the nerves by removing the bone and tissue pressing on them.
Minimally invasive techniques are becoming more popular, offering faster recovery times. Success rates are generally high, with 70-80% of patients reporting significant improvement in symptoms. However, surgery is a major decision. It’s typically reserved for those with severe disability or progressive neurological deficits like foot drop (inability to lift the front part of the foot).
Living With Neurogenic Claudication
Managing this condition is about adaptation. Here are some practical tips:
- Use assistive devices: A walker or cane allows you to lean forward slightly, opening the spinal canal. Don’t view it as a sign of weakness; view it as a tool for independence.
- Modify your environment: Use raised toilet seats and shower chairs to avoid prolonged standing or awkward bending.
- Listen to your body: If you feel the "lead legs" sensation, stop and sit. Pushing through the pain can worsen inflammation.
- Maintain a healthy weight: Extra weight puts more pressure on the spine, exacerbating stenosis.
Remember, neurogenic claudication is manageable. With the right diagnosis and a tailored treatment plan, you can maintain an active lifestyle. The key is understanding your body’s signals and working with healthcare providers who specialize in spine health.
Can neurogenic claudication go away on its own?
It rarely disappears completely without intervention because the underlying structural narrowing remains. However, symptoms can fluctuate. Periods of inflammation may subside, providing temporary relief. Long-term management usually requires active strategies like exercise and posture modification to keep symptoms controlled.
Is walking good for spinal stenosis?
Walking is beneficial if done correctly. Walking on an incline or using a treadmill set to a slight uphill grade encourages a forward-flexed posture, which opens the spinal canal. Flat walking or walking downhill can worsen symptoms by extending the spine. Listen to your body and stop if pain becomes severe.
How long does recovery take after laminectomy?
Recovery varies by individual and surgical approach. For minimally invasive decompression, many patients return to light activities within 2-4 weeks. Full recovery and maximum benefit from surgery can take 3-6 months. Physical therapy is almost always prescribed post-surgery to strengthen core muscles and support the spine.
What foods help with nerve pain?
While no food cures spinal stenosis, an anti-inflammatory diet may help manage symptoms. Focus on omega-3 fatty acids (found in fish, flaxseeds), antioxidants (berries, leafy greens), and vitamin B12 (important for nerve health). Avoid excessive sugar and processed foods, which can increase systemic inflammation.
When should I see a specialist for leg pain?
See a specialist if you experience progressive weakness in your legs, loss of bowel or bladder control (a medical emergency known as cauda equina syndrome), or if pain persists despite rest and over-the-counter medications. Early diagnosis prevents long-term nerve damage and improves treatment outcomes.
