
You take your pain medication, hoping for relief. Instead of comfort, you’re stuck in a cycle of bloating, discomfort, and the dread that you won’t be able to have a normal bowel movement. This isn’t just an unpleasant side effect; it’s Opioid-Induced Constipation, or OIC, a distinct medical condition that affects up to 95% of patients on chronic opioid therapy. Unlike nausea or drowsiness, which often fade as your body adjusts, OIC persists. It doesn’t go away with time, and ignoring it can lead to severe complications or force you to stop your pain treatment entirely.
The good news? You don’t have to live with it. There are specific, evidence-based strategies to prevent OIC before it starts and prescription options that target the root cause rather than just masking symptoms. Here is how to manage OIC effectively, from simple preventive steps to advanced pharmaceutical interventions.
Why Opioids Cause Constipation (And Why Fiber Fails)
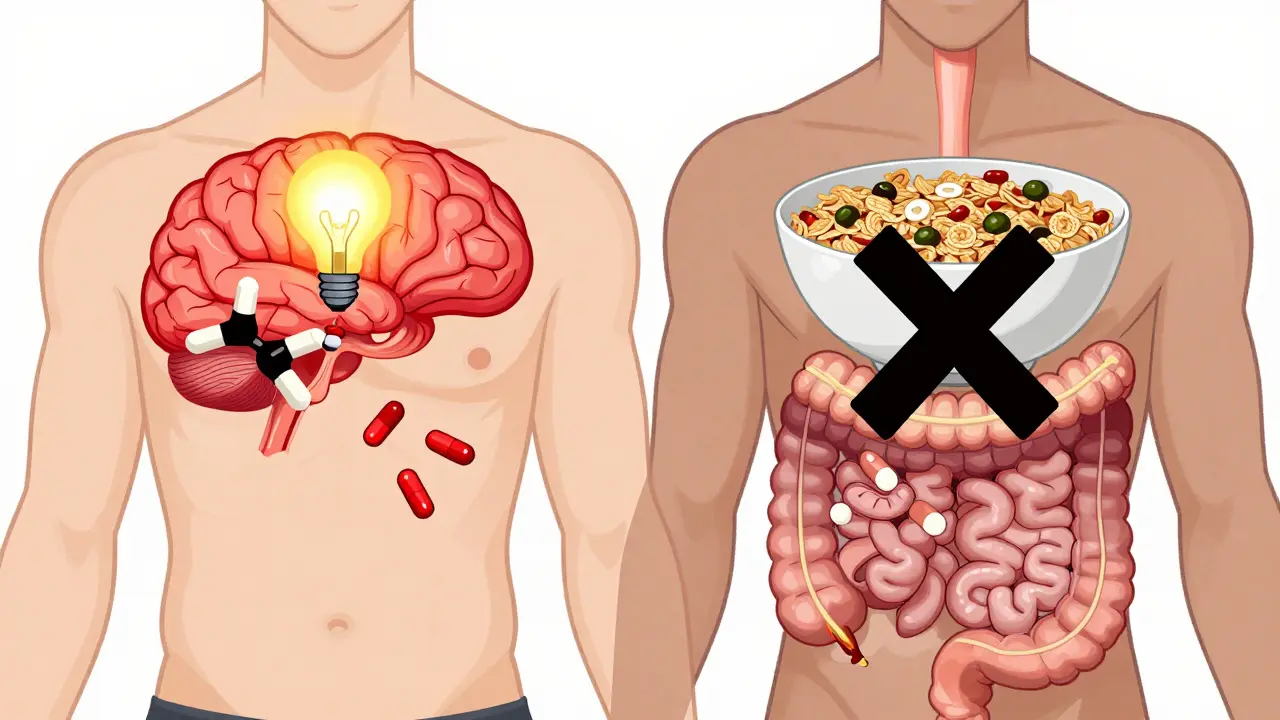
To treat OIC, you first need to understand why it happens. Opioids bind to mu-opioid receptors in your brain to block pain signals. However, these same receptors exist throughout your gastrointestinal tract. When opioids activate these gut receptors, they slow down gastric emptying, reduce intestinal secretions, and increase water absorption from your stool. The result? Hard, dry stools and a sluggish digestive system.
This mechanism is fundamentally different from typical constipation caused by low fiber intake or dehydration. That’s why the standard advice for general constipation-eating more fiber-can actually make OIC worse. According to Dr. J. Camilleri from Mayo Clinic, increasing dietary fiber to 30g/day is often contraindicated in OIC cases. Because opioids inhibit motility, adding bulk via fiber can lead to fermentation, bloating, flatulence, and even fecalomas (hardened masses of stool). If you are taking opioids, skip the extra bran cereal and focus on hydration and targeted medications instead.
Prevention: The First Line of Defense
The most effective way to handle OIC is to prevent it. Clinical guidelines emphasize proactive management starting from day one of opioid therapy. Waiting until you are severely constipated makes treatment much harder.
- Baseline Assessment: Before starting chronic opioids, assess your current bowel function using tools like the Bristol Stool Form Scale. Knowing your "normal" helps you spot changes early.
- Start Laxatives Early: For new patients, clinicians should initiate prophylactic laxative therapy immediately. The goal is a 70-80% response rate within the first week.
- Regular Monitoring: Check your bowel habits weekly. Don’t wait for a problem to arise. If you notice a change in frequency or consistency, adjust your regimen promptly.
- Hydration: While fiber might not help, water is essential. Opioids pull water out of your intestines into your bloodstream. Drinking adequate fluids helps keep stool softer, though it alone rarely solves OIC.
If you are already on opioids and experiencing symptoms, do not assume this is "just part of the process." Untreated OIC leads to significant quality-of-life issues and causes 30-40% of patients to reduce or stop their prescribed pain medication, compromising their pain control.
First-Line Treatments: Over-the-Counter Options
For mild cases or as a starting point, over-the-counter (OTC) laxatives are the standard first-line treatment. However, conventional laxatives fail in 50-75% of OIC cases because they don’t address the opioid receptor binding. Still, they are worth trying under medical guidance.
| Type | Common Examples | Dosage Range | Efficacy in OIC |
|---|---|---|---|
| Osmotic Laxatives | Polyethylene glycol (Miralax), Macrogol | 17-34g daily | Moderate (Preferred first-line) |
| Stimulant Laxatives | Bisacodyl, Senna | Bisacodyl: 5-15mg; Senna: 8.6-17.2mg daily | Moderate (Often combined with osmotics) |
| Fiber Supplements | Psyllium, Methylcellulose | Varies | Low (May worsen symptoms) |
Polyethylene glycol is generally preferred as the initial choice. Stimulant laxatives like senna or bisacodyl are often added if osmotics alone aren’t enough. If you find yourself needing higher doses every few days without relief, it’s time to move to second-line prescription options.
Second-Line Prescriptions: PAMORAs
When OTC laxatives fail, the next step is Peripherally Acting Mu-Opioid Receptor Antagonists, known as PAMORAs. These drugs are designed specifically for OIC. They block opioid receptors in the gut to restore motility but do not cross the blood-brain barrier, meaning they preserve your pain relief while fixing the constipation.
There are three main PAMORAs available, each with unique profiles:
- Methylnaltrexone (Relistor®): Available as a subcutaneous injection. It acts quickly, with many patients reporting relief within 4 hours. It was originally approved for palliative care patients but is now used more broadly. Common side effects include injection-site reactions and abdominal pain. Cost is a significant barrier, with monthly prices ranging from $500-$1,200 depending on insurance.
- Naloxegol (Movantik®): An oral tablet taken once daily. Approved for chronic non-cancer pain, it offers convenience for those who dislike injections. Side effects can include nausea and diarrhea.
- Naldemedine (Symcorza®): Also an oral tablet, naldemedine has shown high patient satisfaction rates (6.8/10 on Drugs.com). It is approved for both adults and, as of March 2023, pediatric patients. About 59% of users report moderate to significant improvement in bowel function.
Clinical trials show PAMORAs have a 40-50% response rate compared to 25-30% for placebo. While expensive, they are highly effective for patients who have failed conventional therapy. Insurance coverage often requires "step therapy," meaning you must prove OTC laxatives didn’t work before getting approval for a PAMORA.

Alternative Prescription: Lubiprostone
If PAMORAs are not suitable or covered, Lubiprostone (Amitiza®) is another FDA-approved option for OIC. It works differently by activating chloride channels in the intestine, increasing fluid secretion and speeding up transit time.
Lubiprostone was initially approved only for women due to limited male enrollment in early trials, though it is effective for men as well. The most common side effect is nausea, occurring in about 30% of patients, followed by diarrhea in 15-20%. It is important to note that lubiprostone is contraindicated with diuretics due to the risk of hypokalemia (low potassium). If you are on other medications, discuss potential interactions with your doctor.
Practical Steps for Patients and Providers
Managing OIC requires a partnership between you and your healthcare provider. Here is a checklist to ensure you are getting the right care:
- Communicate Early: Tell your doctor about any changes in bowel habits immediately. Do not suffer in silence.
- Track Symptoms: Use a simple diary or app to log bowel movements, pain levels, and laxative use. This data helps your provider tailor your treatment.
- Review Medications: Ask if your current opioid dose or type could be adjusted. Sometimes rotating to a different opioid can reduce GI side effects.
- Understand Costs: If prescribed a PAMORA, check with your insurance about prior authorization requirements. Patient assistance programs may be available to help with costs.
- Avoid Self-Medication Risks: While 68% of patients modify their laxative regimens on their own, doing so without guidance can lead to electrolyte imbalances or dependency on stimulant laxatives.
Remember, OIC is a manageable condition. With the right combination of preventive measures, appropriate laxatives, and possibly PAMORAs, you can maintain your pain control without sacrificing your digestive health. Don’t let constipation dictate your quality of life.
Does opioid-induced constipation go away on its own?
No, unlike nausea or vomiting, OIC does not typically resolve as your body adjusts to opioids. It persists throughout therapy and requires active management with laxatives or prescription medications.
Can I eat more fiber to help with OIC?
Generally, no. Increasing fiber intake can worsen OIC by causing bloating and hardening of stool due to reduced intestinal motility. Focus on hydration and medically approved laxatives instead.
What are PAMORAs and how do they work?
PAMORAs (Peripherally Acting Mu-Opioid Receptor Antagonists) are prescription drugs that block opioid receptors in the gut to restore bowel movement without affecting pain relief in the brain. Examples include methylnaltrexone, naloxegol, and naldemedine.
How long does it take for OIC treatments to work?
Injectable methylnaltrexone can provide relief within 4 hours. Oral PAMORAs and laxatives may take several days to establish a regular pattern. Consistency is key for long-term management.
Is OIC dangerous if left untreated?
Yes, untreated OIC can lead to fecal impaction, bowel obstruction, and significant discomfort. It also increases the risk of patients stopping their necessary pain medication, leading to uncontrolled pain.
