
Living with persistent pain often feels like being stuck in a loop. You visit the clinic, get scans, hear that your tissues look "okay," but still hurt when you move. This disconnect between structural damage and pain intensity is where traditional medicine sometimes falls short. That gap has given rise to a powerful approach called Pain Neuroscience Education, which helps people understand that pain is more than just tissue injury.
This concept shifts the conversation from fixing broken parts to calming a hypersensitive nervous system. It’s not about ignoring the pain, but changing how your brain interprets signals. As research from 2023 shows, this method significantly improves function and reduces disability scores in chronic conditions. Let’s explore what this actually means for your recovery journey.
What Exactly Is Pain Neuroscience Education
Pain Neuroscience Education is a therapeutic educational approach that provides individuals experiencing pain with comprehensive understanding of the underlying neurobiology and neurophysiology of their pain experience. Unlike standard advice focusing on rest or ice, this method treats pain as an output generated by the brain based on perceived threat levels. It emerged in the early 2000s when scientists realized structural explanations didn't match patient experiences. Key figures like Adriaan Louw and Lorimer Moseley pioneered methods to explain complex brain functions simply. They moved away from saying your back is "bad" toward explaining how your alarm system might be too sensitive. A standard session lasts between 30 and 45 minutes. During this time, a clinician explains concepts like sensitization using everyday metaphors rather than medical jargon.
The Science Behind the Approach
To understand why this works, we need to look at how your nervous system processes information. Two main concepts drive the logic behind this therapy.
Neuroplasticity and Central Sensitization
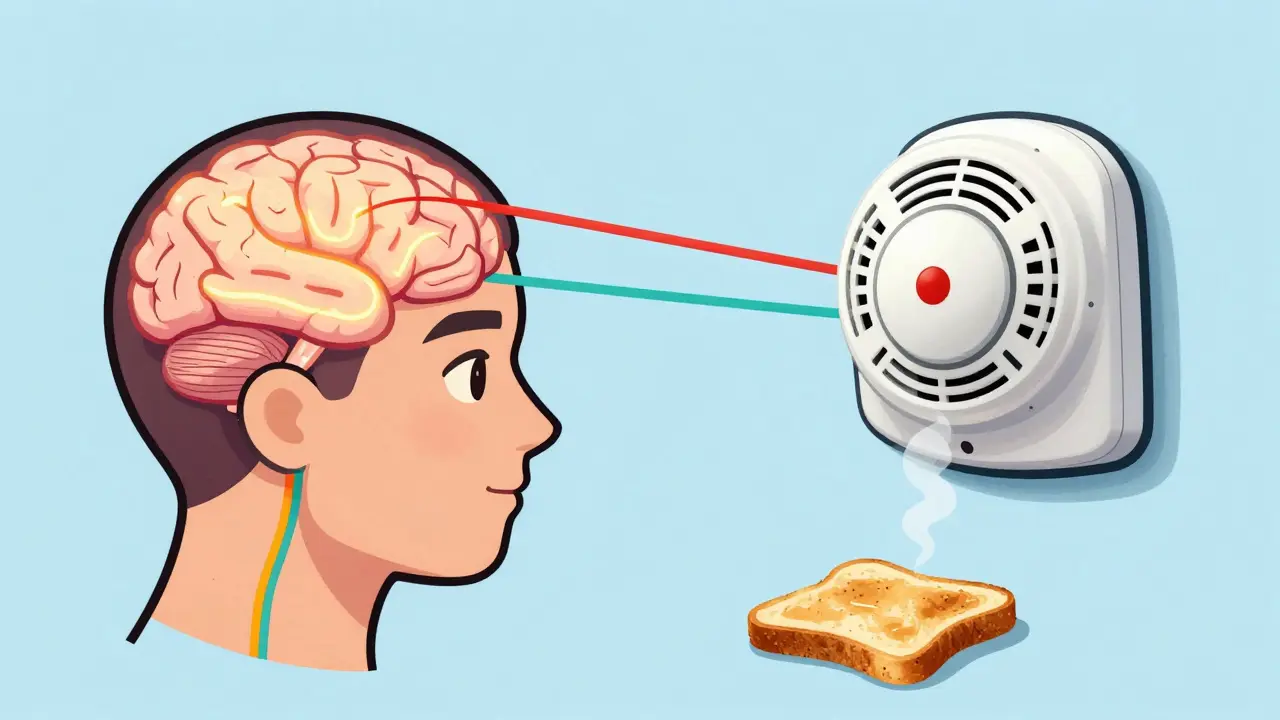
Your brain changes constantly, a trait known as Neuroplasticity. In chronic pain cases, pathways involved in pain signaling can become overactive. Think of it like a fire alarm that goes off when there’s just burnt toast instead of a real fire. This state is called central sensitization. The nerves are sending danger signals even without active tissue damage.
Biopsychosocial Model is another pillar. This framework acknowledges that biological factors, psychological state, and social environment all influence pain. If you believe movement is dangerous because of past injuries, your brain reinforces those neural pathways. Education aims to downgrade the threat value of those movements. Studies using fMRI have shown that after effective education, brain regions associated with threat detection show reduced activation.
How It Compares to Traditional Methods
You might wonder how this stacks up against standard treatments like manual therapy or medication alone. The data suggests a clear difference in long-term outcomes regarding disability.
| Feature | Pain Neuroscience Education | Traditional Biomedical Model |
|---|---|---|
| Primary Focus | Nervous system sensitivity and threat processing | Tissue damage and structural repair |
| Disability Improvement | Average reduction of 12.3% in disability scores | Limited impact on functional movement |
| Long-Term Retention | High knowledge retention with digital reinforcement | Knowledge often fades after acute phase |
| Effect on Catastrophizing | Reduces fear-avoidance behaviors significantly | Often reinforces avoidance due to injury focus |
Data from systematic reviews indicates that combining education with exercise yields better results than either alone. Research shows adding movement strategies increases the benefit by an additional 30 to 40 percent. However, pure education alone still produces clinically meaningful changes in pain intensity averages of roughly 1.7 points on a 0-10 scale.
Who Benefits Most From This Method
This intervention isn't a magic cure for every situation, but it excels in specific areas. It is particularly effective for chronic pain conditions where tissue healing has plateaued. Patients with persistent low back pain, fibromyalgia, or headaches often see significant gains.
Conversely, it shows limited utility for fresh acute injuries where inflammation is high. About 82 percent of studies support its use for chronic issues, whereas fewer than 11 percent show strong benefits for fresh injuries under 6 weeks old. Additionally, cognitive ability matters. If a patient struggles to grasp abstract concepts or has severe cognitive impairment, the educational component becomes harder to process.
Real-Life Impact and Patient Stories
Statistics tell one story, but patient experiences tell another. In online support communities, users frequently discuss shifting their relationship with pain. One documented case involved a nurse suffering from fibromyalgia who utilized a six-session program. She managed to reduce daily medication intake from six pills down to one every three days.
Success usually hinges on the metaphor used. Common analogies include the "smoke alarm" analogy mentioned earlier. If you understand the alarm is sensitive rather than faulty, you stop fearing the sound itself. Some users report feeling empowered to return to hobbies like hiking they feared would cause harm. On average, satisfaction rates hover around 68 percent, slightly higher than cognitive behavioral therapy for pain alone.

Finding the Right Practitioner
Accessing this care requires finding clinicians trained specifically in this methodology. Not every therapist uses these techniques. Look for credentials related to specialized training in pain science. Organizations like the International Spine and Pain Institute offer certification courses for therapists. While no mandatory license exists globally, reputable clinics will openly discuss their use of these educational frameworks.
In Australia, integration into public and private practices is growing rapidly. Insurance rebates often cover these sessions under standard evaluation codes, though coverage varies by provider. When booking an appointment, ask directly: "Does your treatment plan include education on how my nervous system contributes to pain?" This ensures you aren't just getting passive therapies but active retraining of your perception.
Common Concerns and Misconceptions
Skepticism is natural. Many worry this approach implies their pain is "in their head." That is not the case. The pain is real, but the mechanism involves the brain's protective interpretation rather than active tissue damage. Another concern is complexity. Learning neurobiology can seem daunting.
Effective practitioners avoid overwhelming jargon. They use visual aids, handouts, or apps like the 'Pain Revolution' tool to reinforce learning. If you find a session confusing, communicate that immediately. Good therapy adapts to your literacy level and background.
Integrating Concepts Into Daily Life
Education is most powerful when applied practically. Once you leave the clinic, consistency matters. Try grading your activity levels. Instead of pushing through pain, increase movement gradually to prove to your brain that motion is safe. Writing down progress notes can help track changes in pain perception versus intensity.
Combining this mindset with regular exercise creates a synergistic effect. Even simple walking programs reinforce the safety messages delivered during sessions. Consistency in applying these principles leads to sustained improvements in sleep quality, mood, and overall physical capacity.
Is Pain Neuroscience Education suitable for acute injuries?
It is generally less effective for acute pain where tissue damage is the primary driver. Research shows limited benefit for injuries under six weeks old compared to chronic conditions.
Can I do this therapy online?
Yes, digital delivery methods including apps and virtual consultations are increasingly validated and retain high knowledge levels.
Does insurance typically cover these sessions?
Coverage depends on the provider, but many Medicare and private insurers now reimburse education as part of standard physiotherapy evaluations.
Will this replace medication?
It can often reduce reliance on medication by managing pain perceptions, but never stop medication without consulting your doctor first.
How long does a typical session take?
Standard sessions last approximately 30 to 45 minutes and are often integrated alongside movement-based therapies.










It is beneficial to share these insights openly. :) Understanding the difference helps alot in recovery. Often we assume damage equals pain intensity constantly. But the brain processes threat differently than pure signals. :) It empowers folks to take charge of their healing journey. Seeing the logic behind the alarm system really clarifies things. :D Many overlook how much mindset affects recovery speed. Public access to this data is highly valuable for all readers.